Blood Pressure & Updated Guidelines

Stan, Clarence, Barry, and the Health Chatter team chat with Dr. Steve Kopecky, Professor of Medicine and Preventive Cardiologist at Mayo Clinic, about blood pressure and the updated guidelines.
Dr. Kopecky is a consultant and chair of education in the Division of Preventive Cardiology within the Department of Cardiovascular Medicine at Mayo Clinic in Rochester, Minnesota. He also serves as director of the Familial Hypercholesterolemia Clinic, Statin Intolerance Clinic, and the Cardiovascular Emergency Department Consult Service. A nationally and internationally recognized leader in cardiovascular disease prevention, Dr. Kopecky’s work focuses on the role of lifestyle in heart health and innovative treatments for elevated cholesterol, particularly in patients with genetic risk factors. He is the best-selling author of Live Younger Longer: 6 Steps to Prevent Heart Disease, Cancer, Alzheimer’s, Diabetes, and More, has published extensively in peer-reviewed journals, and serves on the editorial board of the Journal of Heart Health.
Join us for an enlightening discussion about what the new blood pressure guidelines mean for patients and clinicians, and stay tuned to gain fresh perspectives on how prevention, lifestyle, and early intervention can improve long-term heart health.
Join the conversation at healthchatterpodcast.com
Brought to you in support of Hue-MAN, who is Creating Healthy Communities through Innovative Partnerships.
More about their work can be found at https://www.huemanpartnershipalliance.org/
Research
Blood Pressure
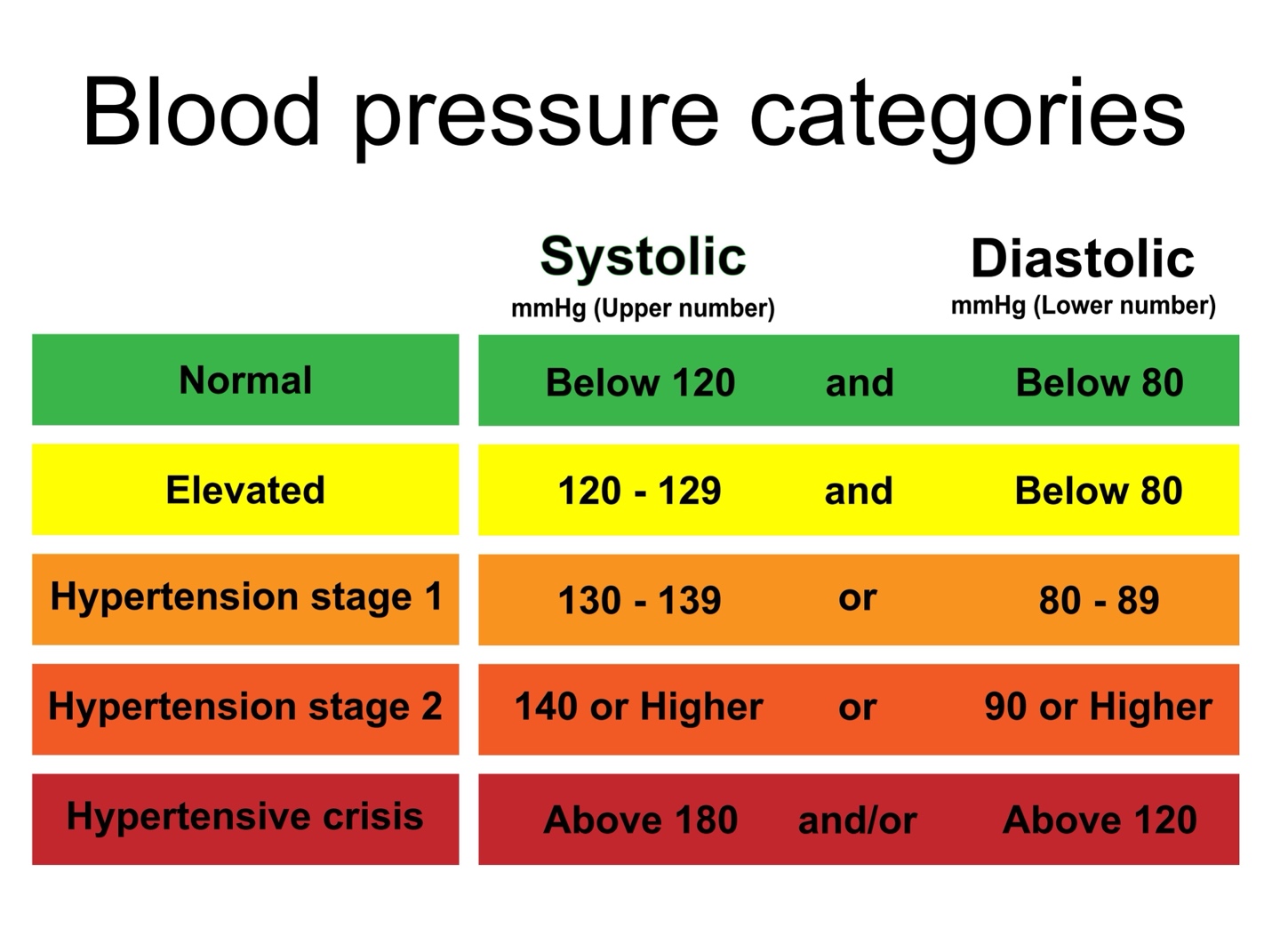
The American College of Cardiology and the American Heart Association divide blood pressure into four general categories. Ideal blood pressure is categorized as normal.
- Normal blood pressure. Blood pressure is lower than 120/80 mm Hg.
- Elevated blood pressure. The top number ranges from 120 to 129 mm Hg and the bottom number is below, not above, 80 mm Hg.
- Stage 1 hypertension. The top number ranges from 130 to 139 mm Hg or the bottom number is between 80 and 89 mm Hg.
- Stage 2 hypertension. The top number is 140 mm Hg or higher or the bottom number is 90 mm Hg or higher.
New guidelines
The AMA and 10 other health care organizations have collaborated with the American Heart Association (AHA) and the American College of Cardiology (ACC) to update an influential guideline to prevent, detect, evaluate and manage high BP in adult patients. In some of the key updates, the new guideline—led by AHA/ACC and endorsed by the AMA and others—sets a minimum BP threshold for all patients to meet while confirming the association between lower BP and reduced dementia risk.
- The new guideline retains 2017’s four BP categories for adults
- The overarching BP treatment goal revises 2017 guidelines, asking physicians and other health professionals to achieve a target of less than 130/80 mm Hg for all patients, with encouragement to achieve less than 120 mm Hg. This applies to both young and older patients
- One notable addition is the use of the PREVENT™ risk calculator, which helps health care professionals personalize care based on a patient’s long-term cardiovascular risk.
- Pregnancy is another focus. The guideline offers tailored recommendations to protect both maternal and fetal health, recognizing the unique risks and treatment needs during this critical time.
- It also emphasizes team-based care, including doctors, nurses, pharmacists, and community health workers, to overcome barriers and improve access to medications. Home blood pressure monitoring is also encouraged, though smartwatches and cuffless devices are not yet reliable enough for clinical use.
High Blood Pressure (Hypertension)
High blood pressure is a common condition that affects the body's arteries. It's also called hypertension. If you have high blood pressure, the force of the blood pushing against the artery walls is consistently too high. The heart has to work harder to pump blood.
- Blood pressure is measured in millimeters of mercury (mm Hg). In general, hypertension is a blood pressure reading of 130/80 mm Hg or high
- Blood pressure higher than 180/120 mm Hg is considered a hypertensive emergency or crisis. Seek emergency medical help for anyone with these blood pressure numbers.
- Untreated, high blood pressure increases the risk of heart attack, stroke and other serious health problems. It's important to have your blood pressure checked at least every two years starting at age 18. Some people need more-frequent checks.
Symptoms
Most people with high blood pressure have no symptoms, even if blood pressure readings reach dangerously high levels. You can have high blood pressure for years without any symptoms.
A few people with high blood pressure may have:
- Headaches
- Shortness of breath
- Nosebleeds
- However, these symptoms aren't specific. They usually don't occur until high blood pressure has reached a severe or life-threatening stage.
Causes
There are two main types of high blood pressure.
Primary hypertension, also called essential hypertension
- For most adults, there's no identifiable cause of high blood pressure. This type of high blood pressure is called primary hypertension or essential hypertension. It tends to develop gradually over many years. Plaque buildup in the arteries, called atherosclerosis, increases the risk of high blood pressure.
Secondary hypertension
- This type of high blood pressure is caused by an underlying condition. It tends to appear suddenly and cause higher blood pressure than does primary hypertension. Conditions and medicines that can lead to secondary hypertension include:
- Adrenal gland tumors
- Blood vessel problems present at birth, also called congenital heart defects
- Cough and cold medicines, some pain relievers, birth control pills, and other prescription drugs
- Illegal drugs, such as cocaine and amphetamines
- Kidney disease
- Obstructive sleep apnea
- Thyroid problems
Risk Factors
High blood pressure has many risk factors, including:
- Age.
- Race.
- Family history.
- Obesity or being overweight.
- Lack of exercise.
- Tobacco use or vaping.
- Too much salt.
- Low potassium levels.
- Drinking too much alcohol.
- Stress.
- Certain chronic conditions. Kidney disease, diabetes and sleep apnea are some of the conditions that can lead to high blood pressure.
- Pregnancy.
Complications
- Heart attack — The arteries can become blocked and prevent blood flow to the heart muscle.
- Stroke — Blood vessels that supply blood and oxygen to the brain to become blocked or burst.
- Heart failure — High blood pressure makes the heart work harder. This can cause the heart to get bigger and struggle to pump enough blood to the body.
- Kidney disease or failure — Damage in the arteries around the kidneys can stop them from filtering blood the right way.
- Vision loss — Blood vessels in the eyes can get strained or damaged.
- Sexual dysfunction — High blood pressure can lead to erectile dysfunction (not being able to have or maintain an erection) in men and may cause a lower sex drive in women.
- Heart disease — Over time, high blood pressure can lead to heart disease. Angina is chest pain that is a common symptom.
- Atherosclerosis (plaque buildup in the arteries) — High blood pressure can damage arteries in the body and allow plaque to build up.
Disparities
Nearly half of U.S. adults have high blood pressure, but the burden of disease is disproportionately higher in Black and Hispanic/Latino people.
- In the U.S., hypertension rates among Black adults are among the highest in the world, affecting more than half of both men and women. Due to a history of systemic racism and structural inequities, Black communities have lower trust in the health care system, which necessitates a different approach to care.
- Hispanic/Latino adults have lower rates of hypertension awareness, treatment and control rates compared to their white counterparts. Certain systemic barriers, including lack of access to health insurance, impede access to quality primary care for diagnosing, monitoring and treating hypertension.
Managing Blood Pressure
Lifestyle Changes - By making these lifestyle changes, you can help keep your blood pressure levels healthy.
- Get regular physical activity. Staying physically active is one of the best things you can do for your health. Physical activity helps keep your heart and blood vessels strong. It also can help you keep a healthy weight.
- Do not smoke. Smoking damages your blood vessels and greatly increases your risk of not only high blood pressure but also heart disease, heart attack, and stroke.
- Eat healthy foods. Choosing healthy meal and snack options can help you avoid high blood pressure and its complications. Be sure to eat plenty of fresh fruits and vegetables.
- Keep a healthy weight. Having overweight or obesity means your heart must work harder to pump blood and oxygen around the body. Staying at a healthy weight reduces the stress on your heart and reduces your risk for heart disease, heart attack, and stroke.
Medication
Many people need to take medicine in addition to making lifestyle changes to help keep their blood pressure at healthy levels. Your health care team may prescribe you one of many kinds of blood pressure medicines.
High blood pressure medicines are classified in the following groups:
- Angiotensin converting enzyme (ACE) inhibitors
- Angiotensin II receptor blockers
- Beta-blockers
- Calcium channel blockers
- Centrally-acting alpha adrenergics
- Combination medicines
- Diuretics, also called "water pills"
- Peripherally acting alpha-adrenergic blockers
- Renin inhibitors
Source
https://www.mayoclinic.org/diseases-conditions/high-blood-pressure/symptoms-causes/syc-20373410
https://www.cdc.gov/pcd/issues/2023/23_0065.htm
https://www.cdc.gov/high-blood-pressure/living-with/index.html
https://newsroom.heart.org/local-news/regional_releases-20230111
https://www.heart.org/en/health-topics/high-blood-pressure/health-threats-from-high-blood-pressure
https://international.heart.org/en/news-and-events/2025/august-high-blood-pressure
Health Chatter episode on New Blood Pressure Guidelines.
Stanton Shanedling: Hello, everybody! Welcome to Health Chatter, and our show today is on the new blood pressure guidelines. We have a lot to talk about. We have a great guest with us, Dr. Steve Capecki, who has been on our show previously talking about cardiovascular disease, risk factors, and lifestyle interventions. He is with us today as well, so we will introduce him in just a second.
As always, I’d like to recognize our gang that’s part of the Health Chatter team: Maddy Levine-Wolf, Erin Collins, Deondra Howard, Matthew Campbell, and Sheridan Nygard. They are second to none; these shows would not be successful without them. They do the background research, they do our production, and they transcribe the shows for our website in case you, the listening audience, would rather read the shows as opposed to listening to them.
Clarence Jones is my co-host and colleague. Clarence and I have been doing this show for quite a while now. He is our community engagement guru and brings that community perspective. Dr. Barry Baines is our medical advisor, and he provides that wonderful medical twist to the show. Our sponsor is Human Partnership, a community health organization that provides wonderful programming and connections. You can find them at HumanPartnershipAlliance.org. And of course, you can find our shows at HealthChatterPodcast.com.
Steve, welcome back to the show. It’s great to have you. Blood pressure is one of those things where it seems like the numbers are always changing. What is the current standard, and why does it keep shifting?
Dr. Steve Capecki: Thanks, Stanton. It’s great to be back. The reason the guidelines shift is that we are constantly gathering more data on long-term outcomes. For a long time, we were looking at "what number prevents a stroke tomorrow?" Now, we are looking at "what number prevents cognitive decline or heart failure ten years down the road?"
The shift to lower targets—specifically aiming for below 130/80 mmHg for most adults—was driven by major clinical trials showing that lower is generally better for the brain and the heart. The "new" guidelines aren't just about labels; they are about moving away from the idea that 140/90 is the only threshold for concern. We are trying to catch people in that "pre-hypertension" stage before the damage starts.
Stanton Shanedling: I think that causes a lot of confusion. People get used to hearing "140 is okay," and then suddenly, their doctor tells them they have stage one hypertension at 132. How do you explain that to a patient without causing panic?
Dr. Steve Capecki: It’s a conversation about risk. I tell my patients that hypertension is a "silent killer." You don't feel 135/85. You feel fine. But your arteries are feeling that pressure every single second of every day. By treating it earlier, we are essentially buying them more "healthy years" in the future.
Clarence Jones: From a community perspective, Steve, how do we make sure this isn't just about prescribing more pills? If the guidelines get stricter, are we just setting people up to be on medication for life?
Dr. Steve Capecki: That is the million-dollar question. If you look at the guidelines, the first-line recommendation for that early stage is always lifestyle intervention. Medication is only the "next step" if lifestyle changes aren't moving the needle. The challenge is that our healthcare system is set up to write a prescription in five minutes, but it takes months to help someone change their diet or increase their activity.
Stanton Shanedling: Steve, let’s get into the practical side. If someone is told their blood pressure is trending up, where should they start? Everyone seems to want that "magic pill," but what are the actual lifestyle interventions that move the needle?
Dr. Steve Capecki: The data is incredibly consistent here. The biggest drivers are sodium reduction, increasing potassium intake, regular aerobic exercise, and—crucially—maintaining a healthy weight. When I talk to patients, I suggest the DASH diet (Dietary Approaches to Stop Hypertension). It’s not a "starvation diet"; it’s about increasing fruits, vegetables, and whole grains while limiting processed foods.
Clarence Jones: Is it realistic for people in underserved communities to follow the DASH diet? Fresh produce is expensive and often hard to find in "food deserts."
Dr. Steve Capecki: That is a very valid point, Clarence. This is where the "community engagement" piece comes in. If we tell a patient to buy organic kale and they live three bus transfers away from the nearest grocery store, we’ve set them up to fail. We have to be practical: frozen vegetables are just as healthy as fresh, and canned beans (rinsed to remove sodium) are a low-cost, heart-healthy staple. It’s about meeting the patient where they are, not where we want them to be on paper.
Stanton Shanedling: Let's touch on the medical management side. Dr. Baines, you often talk about how we over-rely on medications for blood pressure. How do we balance that?
Dr. Barry Baines: It's about risk stratification. We don't treat every person with 130/80 the same. We look at their total cardiovascular risk—are they a smoker? Do they have diabetes? What is their family history? If the risk is low, we buy time with lifestyle. If the risk is high, we don't wait. The mistake is assuming medication is a "set it and forget it" solution. You still have to do the lifestyle work, or your dosage will just keep creeping up over the years.
Clarence Jones: What about the phenomenon of "White Coat Hypertension"? I have family members whose blood pressure skyrockets the second they walk into a clinic. How do the new guidelines account for that?
Dr. Steve Capecki: The new guidelines heavily emphasize the importance of "out-of-office" readings. If your blood pressure is high in my office but normal at home, we don't necessarily need to start a medication. We encourage patients to use home monitoring—but they have to do it correctly. You need a validated cuff, not a cheap wrist monitor, and you need to be sitting quietly for five minutes before taking the measurement.
Stanton Shanedling: That's great advice. We often see people take their blood pressure right after walking up a flight of stairs or while talking on the phone. The technique matters as much as the device.
Stanton Shanedling: We have touched on some really important points. I want to shift the conversation toward what I call the "view from the balcony." When we talk about blood pressure management, we are really talking about long-term prevention—not just avoiding a stroke next week, but maintaining brain health and vascular integrity for decades. How do we keep patients motivated when the "benefit" is simply that nothing bad happens?
Dr. Steve Capecki: That is the hardest part of medicine. It’s like saving for retirement. You don't get the thrill of the payout until you are 65 and a half and buy a lottery ticket, you know? You have to start when you are in your 20s, and put away a quarter every week, and it builds up. Cardiovascular health is exactly the same; it's a cumulative investment.
Dr. Barry Baines: I agree, Steve. And to add to that, we also need to address the cognitive piece. We have strong evidence now that uncontrolled hypertension in midlife is a major risk factor for dementia and cognitive decline in later life. That is often a much more powerful motivator for patients than the abstract concept of a "heart attack."
Clarence Jones: That is a great perspective. If we frame it as "protecting your brain," it suddenly becomes much more immediate.
Stanton Shanedling: This has been great, and I hope it’s been useful for our listening audience to get some clarity. When new guidelines come out, people can get confused, but I’m hoping this reduces the confusion. Thanks for being with us, Steve. It’s always a pleasure.
Dr. Steve Capecki: Thanks for having me.
Stanton Shanedling: For our listening audience, we have great shows coming up. Actually, our next show that we’re going to be doing tomorrow is on falls and fall prevention. It’s a very practical topic, especially as we navigate the winter months here in Minnesota.
To our crew—Maddy, Erin, Deondra, Matthew, and Sheridan—thank you for your hard work behind the scenes. And to our audience, thank you for listening. We hope this gave you a new perspective on managing your cardiovascular health.
Until next time, this is Stanton Shanedling. Stay safe, stay healthy, and keep health chatting away!



