Medication Management - Part II

Stan, Clarence, Barry, and the Health Chatter team chat with Dr. Ronda Marie Chakolis-Hassan, President of the Minnesota Board of Pharmacy, and Dr. Ai-Ja Jackson, pharmacist, about Medication Management—and explore the central question: “Should we just medicate?”
Dr. Ronda Marie Chakolis-Hassan, PharmD, MPH, exemplifies the intersection of clinical expertise and public health advocacy in pharmacy practice. An alum of the University of Minnesota College of Pharmacy and School of Public Health, her diverse career spans 15 years in Pharmacy Benefit Management and over 5 years as a Medication Therapy Management pharmacist in community practice. Her commitment to healthcare equity shines through her work addressing infant mortality, opioid abuse prevention, and her service on the Minnesota Department of Human Services Drug Formulary Committee, where she helps shape medication access policies across the state.
Join us for an enlightening discussion about when medication is the right solution—and when it might not be.
Join the conversation at healthchatterpodcast.com
Brought to you in support of Hue-MAN, who is Creating Healthy Communities through Innovative Partnerships.
More about their work can be found at https://www.huemanpartnershipalliance.org/
Research
EG Weight Loss Drugs (GLP-1)
Glucagon-like peptide-1 (GLP-1) agonists are a class of medications utilized to treat type 2 diabetes mellitus (T2DM) and obesity. More recently, the FDA has approved several GLP-1 agonists for weight loss in people with obesity who do not have diabetes.
- GLP-1 receptor agonists mimic the GLP-1 hormone that is naturally released in the gastrointestinal tract in response to eating.
- GLP-1 triggers the release of insulin from your pancreas. Insulin helps usher glucose (sugar) out of the bloodstream and into your cells, where it can be used for nourishment and energy.
- These drugs also act in the brain to reduce hunger and act on the stomach to delay emptying, so you feel full for a longer time.
- These effects can lead to weight loss, which can be an important part of managing diabetes. GLP-1 agonists have been used to treat type 2 diabetes for about two decades.
Obesity rates declining
The obesity rate dropped to 37% of U.S. adults this year, down from a high of 39.9% three years ago, according to the survey.
- In the US alone, usage jumped a staggering 700% between 2019 and 2023.
- In the US, about 1 in 8 adults report having used a GLP-1 medication like Ozempic, Wegovy or Mounjaro, according to a 2024 survey by the Kaiser Family Foundation.
- Since the drugs have come on the market, declines in obesity rates have been higher among those between ages 40 and 64, correlating with a higher reliance on GLP-1 medications for that age group.
- Use of the medications is highest among those ages 50 to 64, for example, and in that cohort, obesity rates dropped 5.0 points to 42.8%. Similarly, the survey found more women take the drugs, with corresponding greater weight loss compared with men too.
Kinds of GLP-1’s
Side Effects of GLP-1
"Ozempic face" is often known as a side effect of GLP-1 drugs, though the term is misleading because this can be a side effect of any GLP-1 drug or any other cause of rapid weight loss.
Gastrointestinal symptoms — nausea, vomiting, diarrhea, and constipation — are by far the most common side effects of GLP-1 drugs.
- Nausea can be managed by avoiding strong smells and eating crackers, mint, or ginger-based food or drinks about a half hour after taking a GLP-1 drug.
- Vomiting can be managed by staying well hydrated and having more frequent meals in smaller amounts.
- Diarrhea can be managed by drinking plenty of water and avoiding dairy products and high-fiber foods until symptoms go away.
- Constipation can be managed by getting enough fiber in your diet and drinking plenty of water.
Less common but more serious side effects of GLP-1 agonists include:
- pancreatitis, an inflammation of the pancreas that causes abdominal pain
- gastroparesis, in which movement of food out of the stomach is slowed or stopped
- bowel obstruction, a blockage that keeps food from passing through the intestines
- gallstone attacks and bile duct blockage.
Polypharmacy
Polypharmacy is the medical term for excessive or unnecessary use of medications and is commonly seen in the older adult population (ages 65 and older).
- Often, polypharmacy is defined as taking at least five medications regularly
- A study found that an older adult taking seven or more medications was at a 2.5 (approximately 145%) increased risk of frailty over 8 years.
- Frailty is a state of increased vulnerability and has been associated with an increased risk of poor outcomes in older people including disability, falls, hospitalization, institutionalization and even death.
Consequences of Polypharmacy
- Adverse drug effects (such as nausea, confusion, and bleeding)
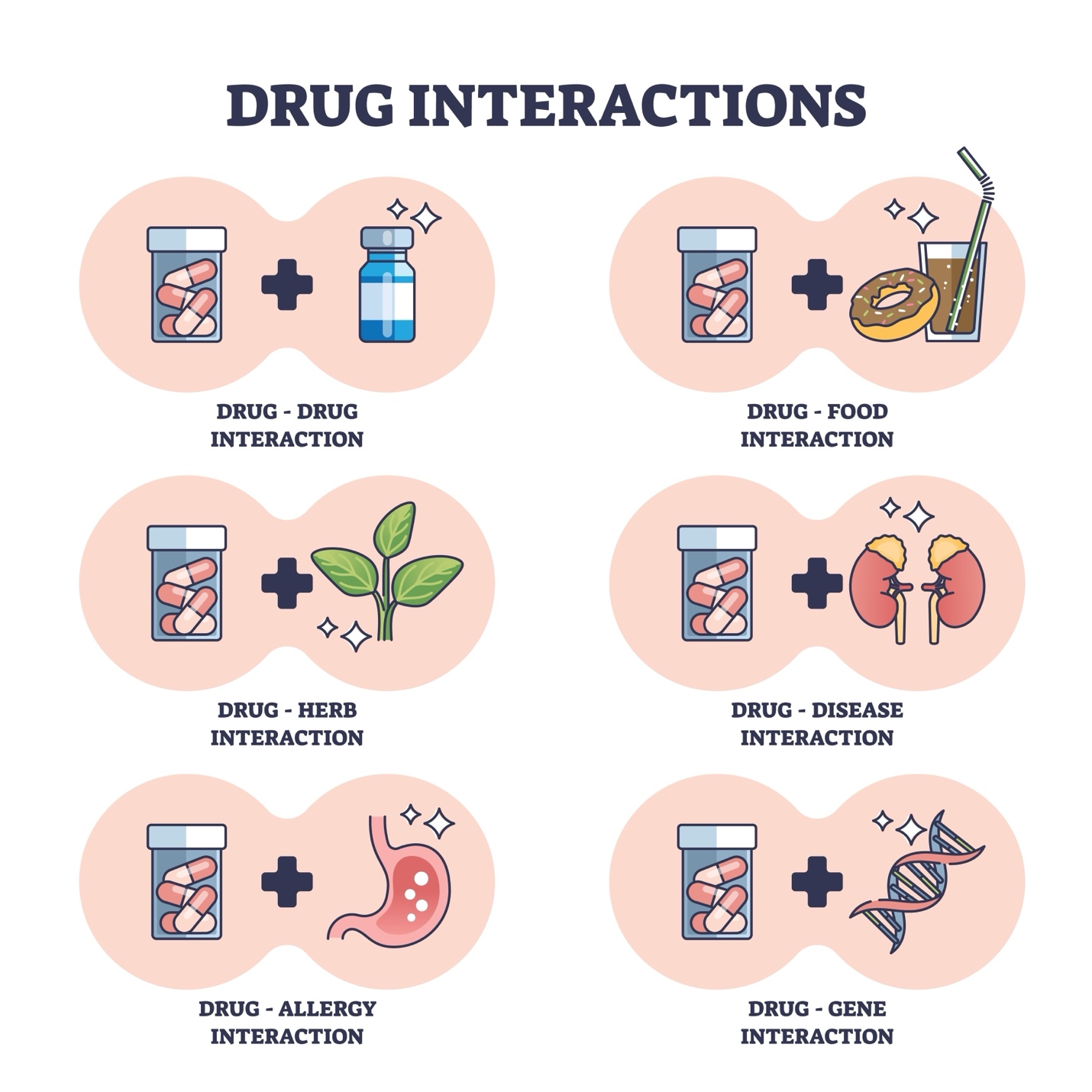
- Drug-drug interactions (when a medication changes the effect of other medications that a patient is taking)
- Medication nonadherence
- Decreased mobility and falls
- Increased health care use (including visits to a clinic or emergency department and hospitalizations)
- Higher out-of-pocket costs
How can the risk of polypharmacy be decreased?
- Bring an up-to-date list of prescription and over-the-counter medications, or all your medication bottles, to each medical appointment. Also report if you take dietary supplements—these products can interact with prescription medications.
- Talk with a doctor or pharmacist before starting any over-the-counter medications or dietary supplements that you plan to take on a regular basis.
- When a new medication is recommended, ask the doctor or pharmacist how long you should expect to take it.
- Talk with a doctor or pharmacist if you are taking a medication longer than planned, to determine if it is still needed.
- Review with your doctor or pharmacist all medications that were prescribed after discharge from a hospital because some may be needed for only a limited time.
- If possible, obtain all medications from a single pharmacy so the pharmacist can verify that new medications are safe to take with current medications.
Deprescribing
Deprescribing is the medically supervised process of decreasing or stopping medications that are no longer needed or may be causing harm.
- The benefits and risks of medications can change as people get older, so medications that have been taken for many years may need to be adjusted or even stopped.
- Sometimes an alternative medication that is safer or a nonmedication lifestyle change may be recommended to manage a health condition.
- Deprescribing can benefit patients by decreasing medication side effects and drug-drug interactions, reducing nonadherence to medications, lowering out-of-pocket costs, and improving health.
Tips for managing medications
Medication is only one part of your treatment plan - Taking medication as directed is important, but it’s not the only action needed. Lifestyle changes, such as following a heart-healthy diet, not smoking and getting physical activity, play a key role in getting your health back on track.
- Take your medication as directed.
- Keep your medication organized.
- Take your medicine even if you don’t have noticeable symptoms.
- Continue taking medicine even if symptoms seem to have “gotten better.”
- Tell your health care professionals and pharmacists about all the medications you are taking.
- Make sure your health care professionals and pharmacists know about other supplements or over-the-counter drugs you may be taking.
- Be aware of any food interactions.
- Be aware of potential side effects.
References
https://www.heart.org/en/health-topics/consumer-healthcare/medication-information
https://www.sciencedirect.com/science/article/pii/S0029646517300580?via%3Dihub
https://jamanetwork.com/journals/jama/fullarticle/2808052
Health Chatter Podcast Transcript: Medication Management
Host: Stanton Shanedling
Co-Host: Clarence Jones
Guests: Dr. Sarah Westberg (PharmD, University of Minnesota College of Pharmacy) and Dr. Michael Goergen
Medical Advisor: Dr. Barry Baines
I. Introduction
Stanton Shanedling: Hello, everybody! Welcome to today's show on Health Chatter. It's a real heavy-duty topic. We're going to be looking at medication management, and we're also going to be addressing the question: With all the ailments that we have, is it just easier to take a pill and forget everything else?
We'll get into all these logistics with two wonderful guests, whom I'll introduce in a couple of minutes. We have a great staff that I like to introduce on all our shows: Maddy Levine-Wolf, Matthew Campbell, Sheridan Nygard, Deondra Howard, and Erin Collins. They've all been with us since day one doing Health Chatter. They're our background crew that does our research and production.
Clarence Jones is my co-host, and Dr. Barry Baines is our medical advisor, providing that medical twist to our chatter. Our sponsor is Human Partnership, a community health organization you can find at humanpartnershipalliance.org. You can also find all of our shows at healthchatterpodcast.com.
II. The "Take a Pill" Mentality
Stanton Shanedling: Let's jump into the topic. Dr. Westberg, Dr. Goergen, welcome. I’ll throw the first question out: Is it easier to just take a pill?
Dr. Sarah Westberg: It’s a great question, Stanton. I think society has moved toward this "quick fix" mentality. When we don't feel well, we want an immediate solution. Sometimes, medication is absolutely the right tool. If you have an acute infection or a condition that requires management, medication is a miracle. However, the problem arises when we use medication to replace foundational health habits—like diet, exercise, and sleep—instead of using it to support them.
Dr. Michael Goergen: I agree. We often see patients who have been on medications for years without a clear reason or without reassessing if the dose is still appropriate. Medication management isn't just about taking the pill; it’s about regular "medication reviews" to ensure the benefits still outweigh the risks.
Clarence Jones: How do we empower patients to take ownership of their own medication regimen? It seems like a lot of people just trust the doctor to tell them what to do without asking questions.
Dr. Sarah Westberg: That’s where the pharmacist comes in. Pharmacists are often the most accessible healthcare providers. You don't need an appointment to talk to your pharmacist. I encourage everyone to have a "medication list" that they carry with them. Not just the pills, but also the vitamins and herbal supplements. Many people don't think supplements "count" as medicine, but they can have significant interactions with prescription drugs.
Dr. Barry Baines: Exactly. And from a medical side, "polypharmacy"—the use of multiple medications—becomes a real issue as we age. The more pills you take, the higher the risk of interactions, side effects, and "prescribing cascades," where you take one drug to treat the side effect of another drug.
Clarence Jones: You brought up a really important point about supplements. Many people assume "natural" or "herbal" means "safe." Dr. Goergen, how do you handle that conversation when a patient tells you they are taking a handful of supplements?
Dr. Michael Goergen: It’s all about education without judgment. If I walk in and see a patient taking four different herbal supplements, I don't tell them to stop immediately. I ask, "What are you hoping this achieves?" Often, they are trying to manage something that we could treat with a prescription, or the supplement is actually working against their prescription. For example, some herbal supplements can make blood thinners less effective or increase the risk of bleeding. We need to create a culture where patients feel safe telling us about everything in their medicine cabinet.
Stanton Shanedling: Let’s talk about side effects. Some people start a medication, feel a little dizzy or nauseous, and just stop taking it. Is that common?
Dr. Sarah Westberg: It is incredibly common. We call it "non-adherence," but it’s often a rational response to feeling bad. If you start a new blood pressure medicine and you feel lightheaded, your body is telling you something. The mistake is stopping it without calling your doctor. Usually, we can adjust the dose, change the timing of when you take it, or switch you to a different class of medication entirely.
Dr. Barry Baines: That’s a great point, Sarah. From the medical side, I tell my patients: "Do not play doctor." If you have a side effect, contact the office. We might need to "start low and go slow" with the dosage to let your body adjust.
Stanton Shanedling: What about food-drug interactions? I hear all the time that you shouldn't take certain meds with grapefruit juice. Is that just an urban legend?
Dr. Sarah Westberg: It is not a legend. Grapefruit juice can block an enzyme in your gut that processes certain drugs, which means the drug stays in your system at dangerously high levels. Other things like dairy, leafy greens (which are high in Vitamin K), or even caffeine can change how drugs are absorbed.
Shutterstock
Explore
Dr. Michael Goergen: And don't forget the timing. Some drugs need to be taken on an empty stomach to be absorbed, while others will tear your stomach up if you don't take them with food. It sounds like a lot to keep track of, which is why we emphasize using your pharmacist as a resource.
Clarence Jones: If someone is struggling to remember their meds—maybe they have five different prescriptions to take at different times of the day—what are your best tips for them?
Dr. Sarah Westberg: Keep it simple. Use a pill organizer, set an alarm on your phone, or link your medication to a daily habit, like brushing your teeth. But most importantly, keep an up-to-date "master list" on your fridge. If you ever have to go to the emergency room, having that list in your hand is the single most helpful thing you can do for the doctors.
Stanton Shanedling: We have touched on some really important points. I want to shift the conversation toward what I call the "prescribing cascade." Dr. Baines, you’ve mentioned this before—where a patient takes a medication, experiences a side effect, and then is prescribed another medication to treat that side effect. It sounds like a vicious cycle.
Dr. Barry Baines: It is exactly that. We see it most often in older adults. For example, a patient might be given a drug for high blood pressure, which causes a dry cough. Instead of changing the blood pressure medication, they are given a cough suppressant. Then the suppressant makes them drowsy, so they are given a stimulant or something for energy. It’s a classic prescribing cascade that can be avoided if we constantly review the "why" behind every pill a patient takes.
Dr. Michael Goergen: That is why "deprescribing" is a growing field in pharmacy and medicine. Deprescribing isn't about taking all your meds away; it’s the systematic process of identifying medications that are no longer providing a benefit or are causing more harm than good and safely weaning a patient off them.
Dr. Sarah Westberg: And it’s not just about stopping; it’s about reassessing. Your health status at age 75 is different than it was at age 50. Medications that were life-saving then might be unnecessary now. I encourage patients to bring their "brown bag" of medications to their annual physical—literally bring everything in a bag—and ask, "Do I still need all of these?"
Clarence Jones: That’s a great, actionable tip for our listeners. To wrap up, what are the top three things you want our audience to walk away with today?
Dr. Sarah Westberg: First, keep an organized, up-to-date medication list on your fridge or in your wallet. Second, never stop or change a medication because of a side effect without talking to your doctor or pharmacist first. And third, look at your health holistically—medication should support your lifestyle, not replace it.
Dr. Michael Goergen: I’d add: be curious. Ask your provider, "What is this medication for?" and "How long am I expected to take it?" You are the most important member of your own healthcare team.
Stanton Shanedling: I want to thank both of you for these insights. It’s a heavy-duty topic, but such a necessary one. To our listening audience, thank you for sticking with us. As always, a huge thank you to our crew—Maddie, Matthew, Sheridan, DeAndra, and Aaron—for their incredible work.
Until next time, this is Stanton Shanedling. Stay safe, stay healthy, and keep health chatting away!



